PEDIATRIC PATIENTS
1. SCANNING TECHNIQUE
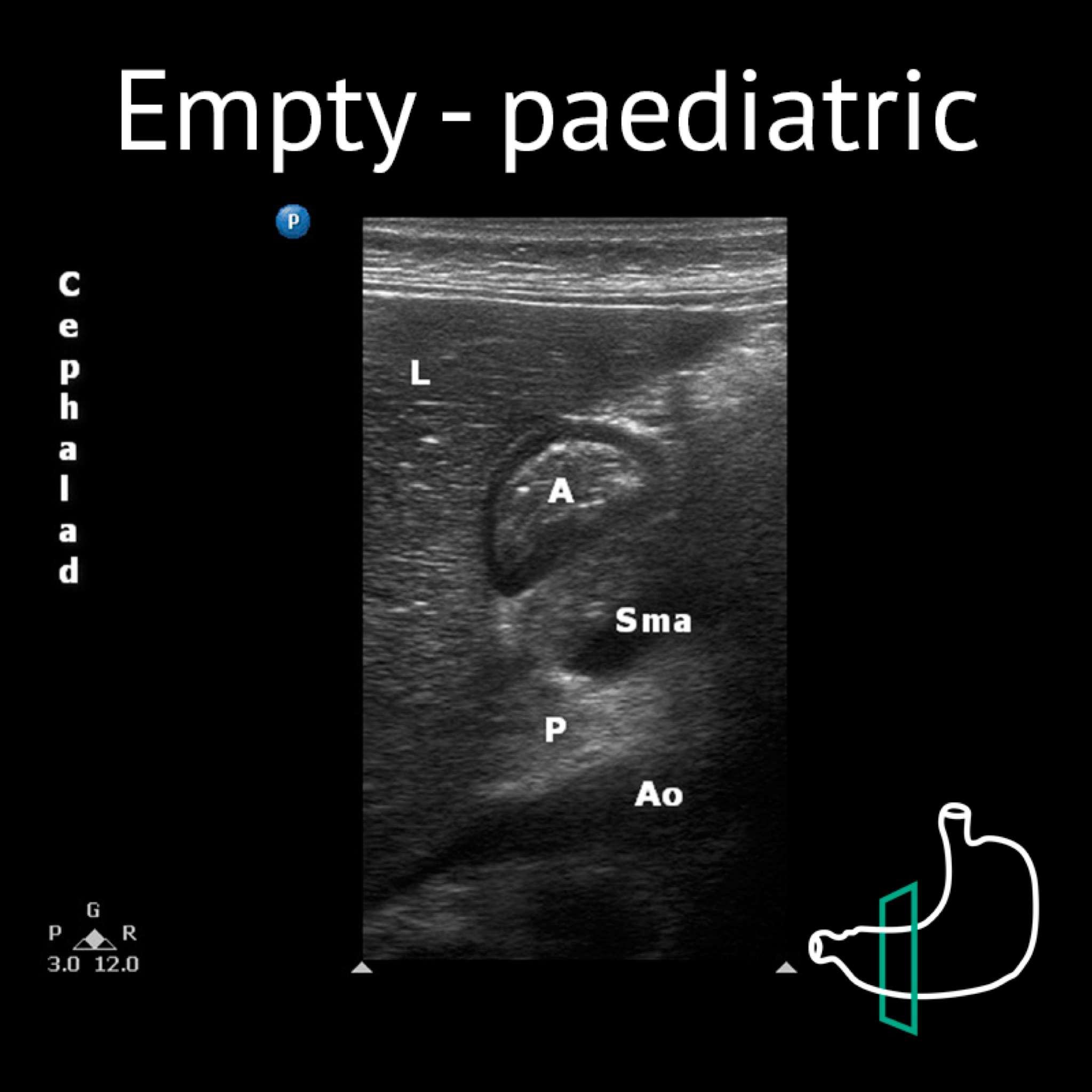
1. Babies are often uncooperative/crying; it may be difficult to ascertain perfect images.
2. In younger/smaller patients (< 30 kg) a high-frequency linear transducer provides the best images.
- The figure below shows the empty antrum of children (RLD) using a high-frequency transducer
3. In older/bigger children, a low-frequency curvilinear transducer may be required
- An 11-year-old patient (23.2kg, 1.28 mL/kg of fluid). The antrum appears empty in supine position and distended with hypoechoic content in the right lateral decubitus (RLD), consistent with a grade 1. (Picture below)
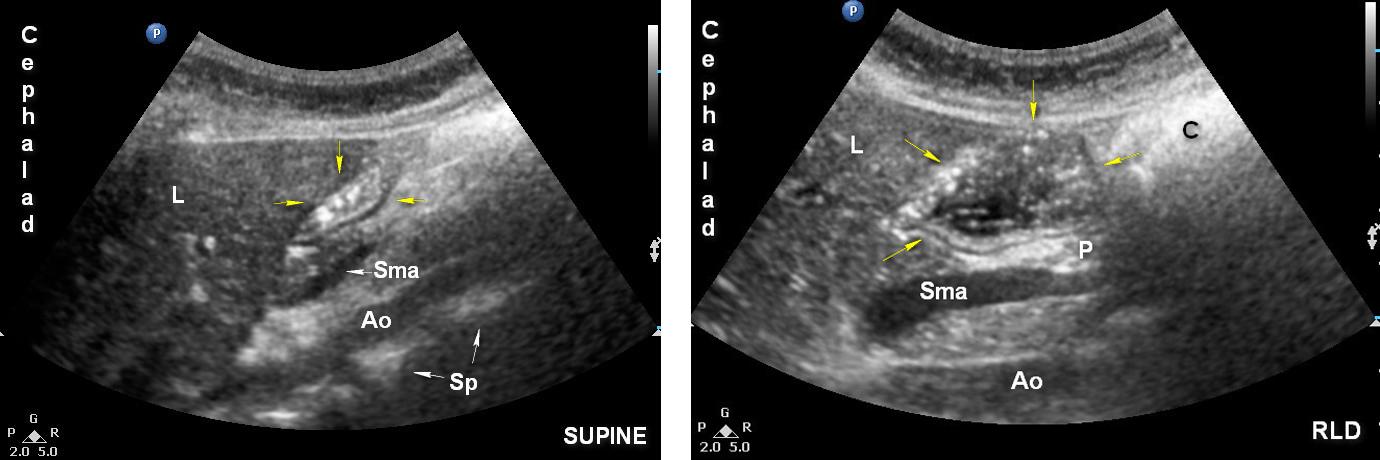
Legend: Ao: aorta A: antrum; C: colon; L: liver; P: pancreas; Sma: superior mesenteric artery; Yellow arrows: antrum
2. GASTRIC VOLUME ASSESSMENT
- Gastric volume may be calculated based on antral CSA and the patient’s age
- The following model has been developed for children based on a cohort of 100 fasted children between the ages of 11 months and 17 years old
VOLUME = -7.8 + (3.5 X RLD CSA) + (0.127) X AGE (MONTHS)
- The upper limit of normal fasting volume in children is 1.1–1.2 mL/kg
- A similar 3-point grading system as described for adults (link) can be used
- Higher grades correlate with higher volumes

3. NEONATES AND PYLORIC STENOSIS
Gastric PoCUS allows us to ensure an empty stomach prior to induction and has a clear impact on anesthetic management.
4. CUT-OFF VALUES
Coming soon
5. NG TUBE INSERTION
Coming soon
