PREGNANT PATIENTS
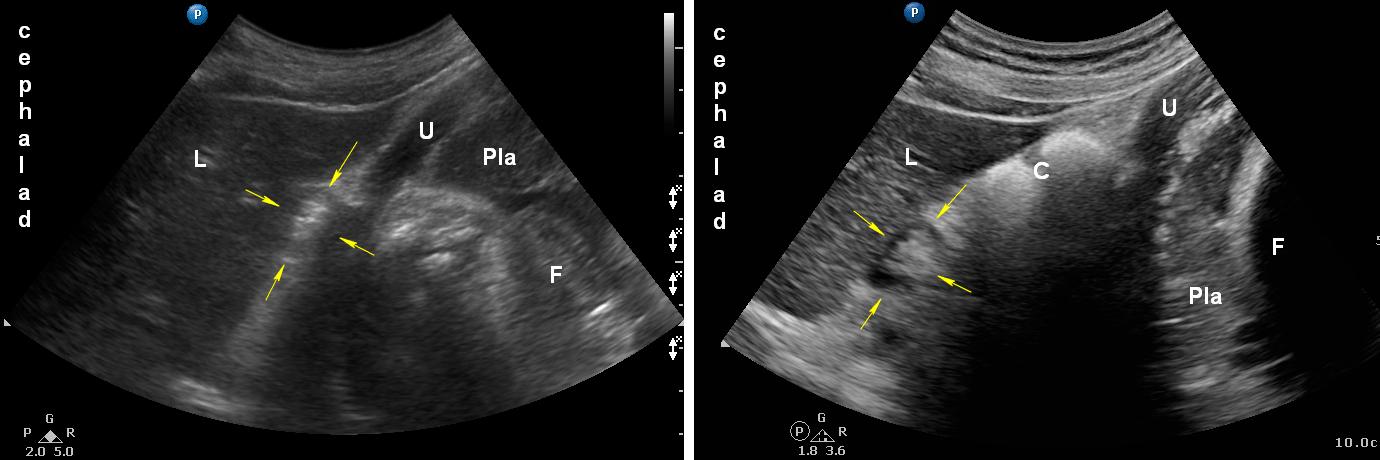
Legend: C: colon; F: foetus; L: liver; P: pancreas; Pla: placenta; U: uterus wall; Yellow arrows: empty antrum.
Identification of the antrum can be more difficult in pregnant patients due to:
- The gravid uterus (and moving fetus)
- The stomach is displaced more cephalad and to the right compared with non-pregnant subjects
- Fast and shallow breathing
- Hyperdynamic circulation
- More difficult epigastric probe placement (steep angle between xyphoid and abdomen)
Visualization can be optimized through:
- Semi-recumbent and right lateral decubitus positions
- Slight manual displacement of the gravid uterus
- Ask the patient to take a slow deep breath and hold her breath at end-expiration
Two mathematical models to estimate total gastric volumes in pregnant patients have been proposed (Arzola et al., 2018; Roukhomousky et al., 2018).
However, based on its internal validity and use of NG suction on gold standard, we propose using the validated Perlas model until further notice.
Qualitative ultrasound assessment accurately determines the type of gastric content (empty, clear fluids, or solid). The sensitivity of the test is highest for solid vs. fluid or empty states.
Non-laboring fasting women at term (e.g. elective C-sections) have similar baseline gastric volume (and antral grade distribution) to the non-pregnant adult population.
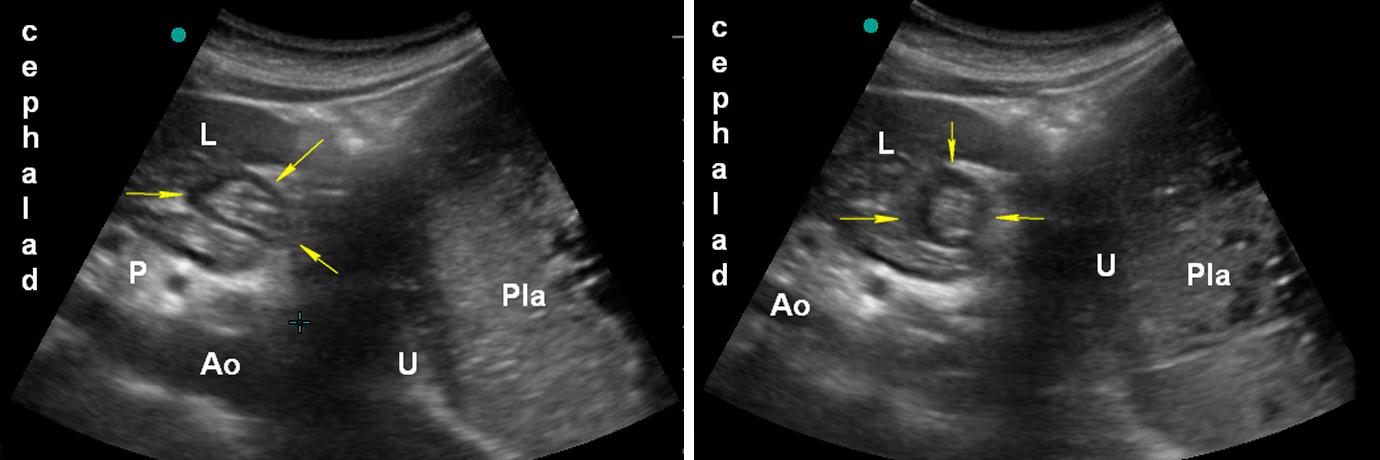
Legend: Ao: aorta; F: foetus; L: liver; P: pancreas; Pla: placenta; U: uterus wall; Yellow arrows: empty antrum.
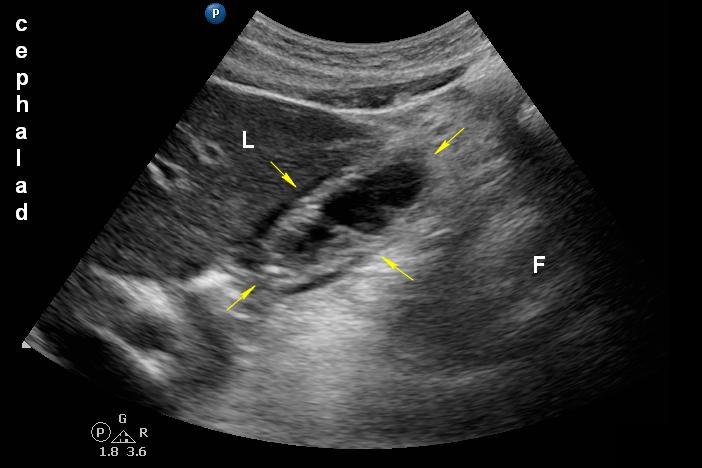
Legend: F: foetus; L: liver; Yellow arrows: fluid filled antrum.
