
4. TYPE OF GASTRIC CONTENT

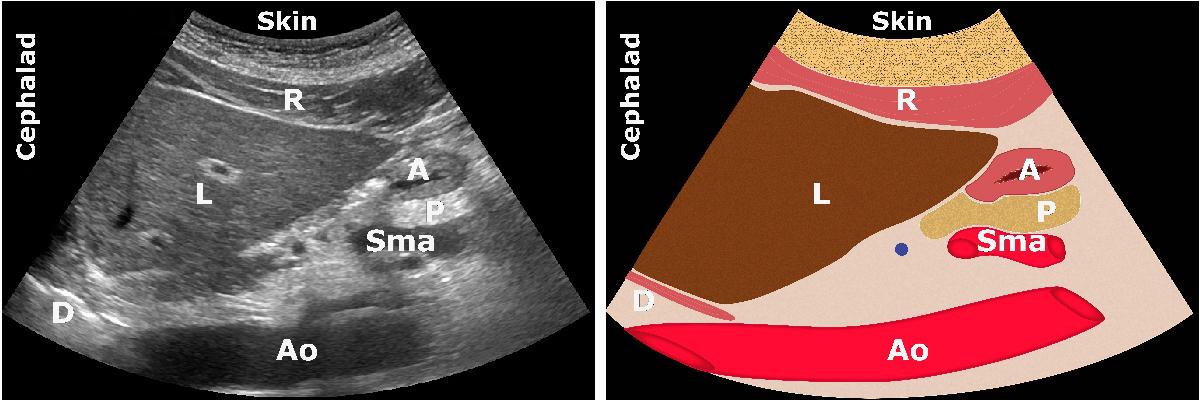
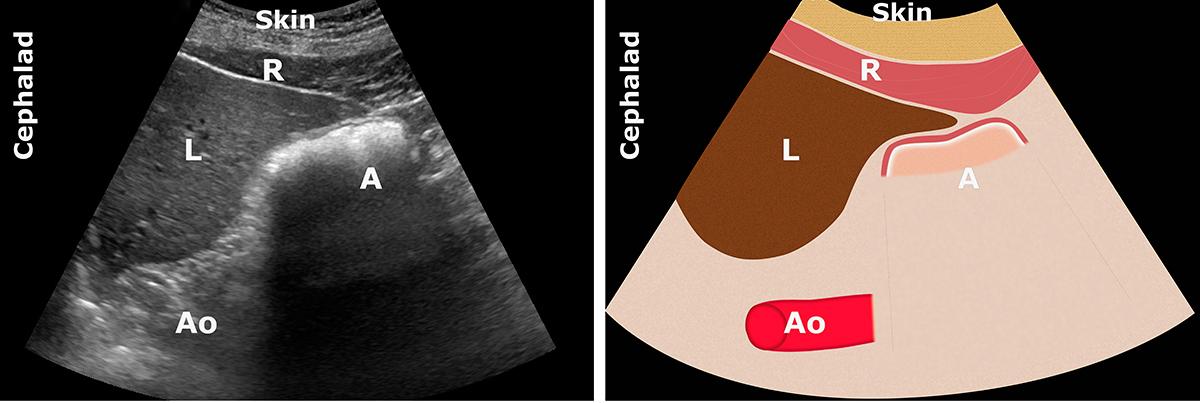
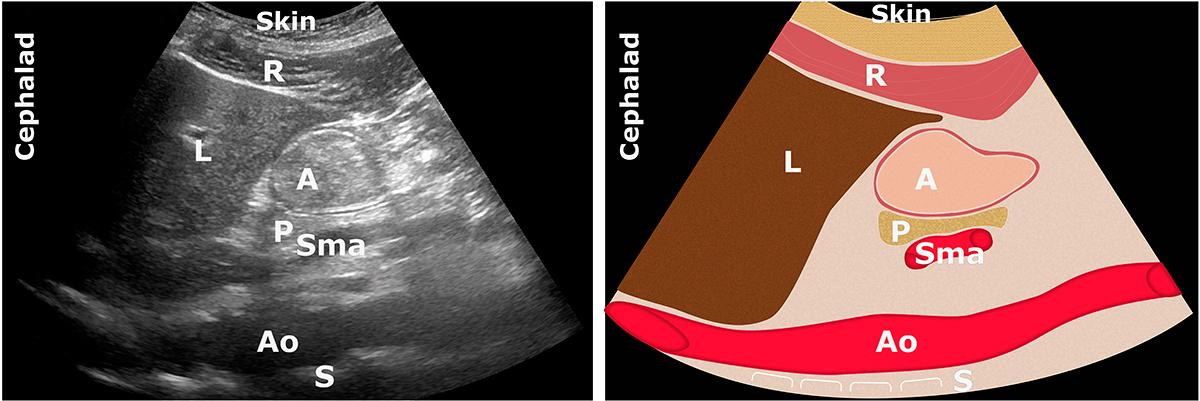
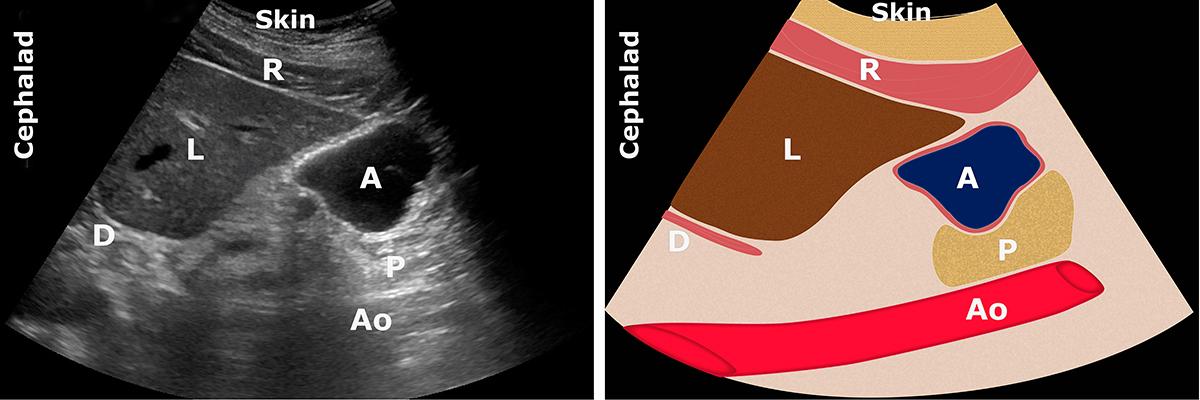
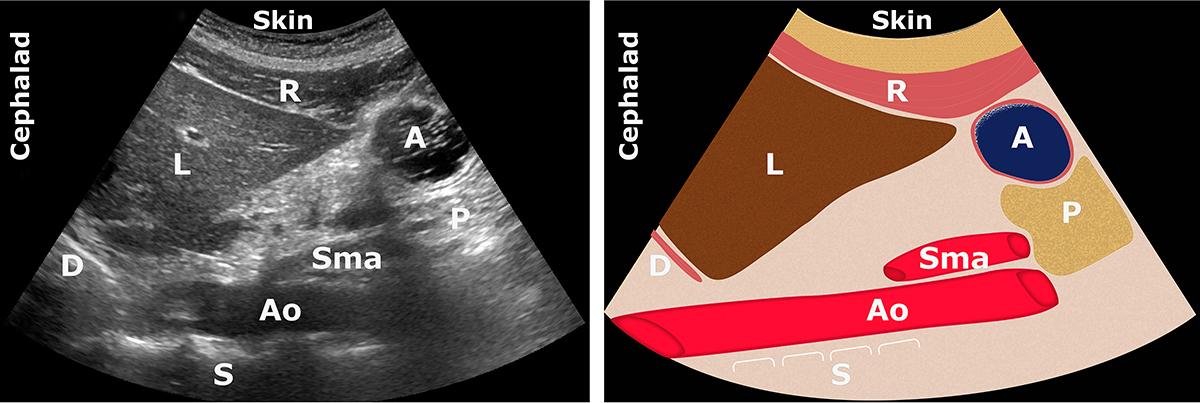
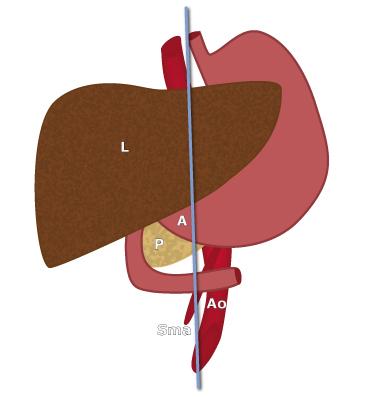
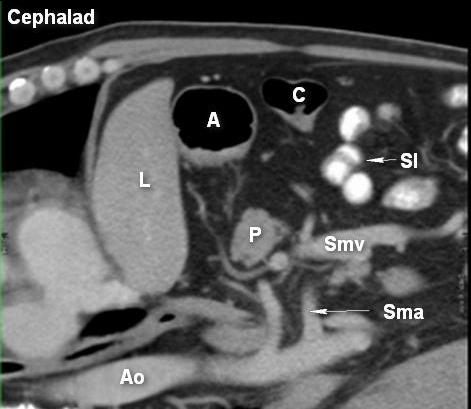
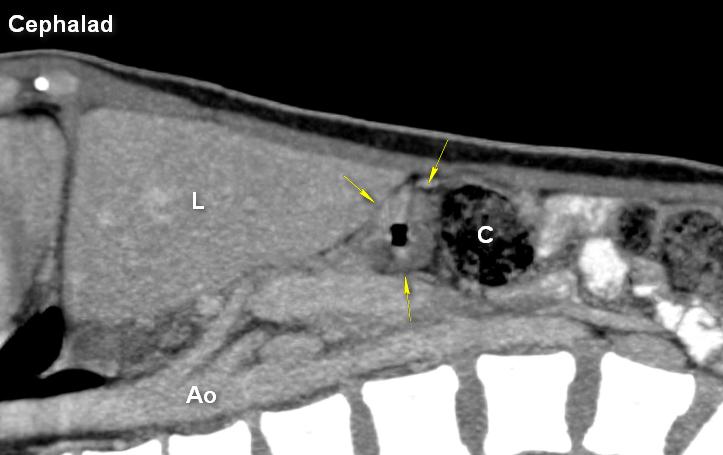
A: antrum; Ao: aorta; D: diaphragm; L: liver; P: pancreas; R: rectus abdominis muscle; Sma: superior mesenteric artery
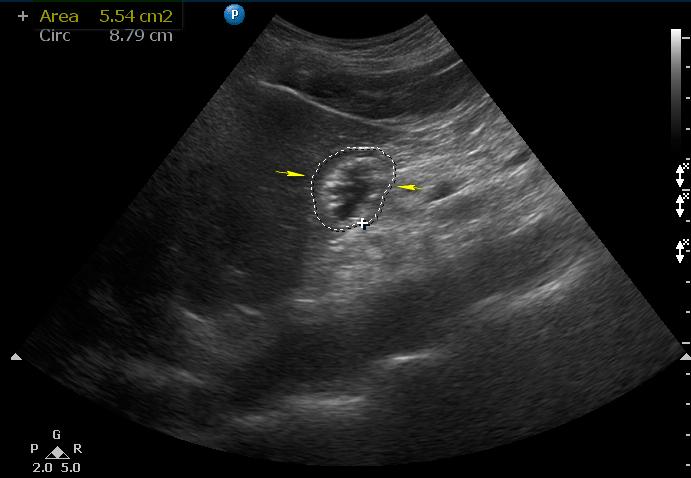
- The antrum has no appreciable content in both supine and RLD (Grade 0 antrum)
- It appears flat and collapsed or with a round-to-ovoid shape (“bull’s eye” or “target” pattern)